
4·
9 days agoIf I use your math of 99.999% dying, only ~80,000 people will survive, not millions…
If I use your math of 99.999% dying, only ~80,000 people will survive, not millions…

It’s down 10% which is the literal definition of decimated!
Trump and Vance, as of today, are just private citizens.
JD Vance is a sitting US senator.

*CUSMA, or NAFTA2, electric boogaloo
I mean, strictly speaking probably plankton, but I’m picking up what you’re putting down!
That’d be the witchiest!
Thank you for introducing me to Wilhoit’s Law:
Conservatism consists of exactly one proposition, to wit: There must be in-groups whom the law protects but does not bind, alongside out-groups whom the law binds but does not protect.

I MUCH prefer them to be caramelized. It just takes me like an hour or two
Have you ever tried the trick where you add baking soda to accelerate the Maillard reaction? Just a small pinch for a couple of onions, and you’re done in 15min or so. Too much and not as tasty.

To properly answer, we need to define what we mean as “airborne” which has gotten a bunch of people very upset recently. Prior to the COVID pandemic, the transmission model for respiratory viruses focussed on 3 distinct models of transmission:
COVID was presumed to only be transmitted through the first 2 methods. But weird things were observed, where transmission occurred when people (or ferret model experiments) were separated by barriers through which ballistic droplets couldn’t pass, like air ducts with multiple 90° bends. People also got sick after being in rooms many minutes after infected people had been present, long after ballistic droplets would have harmlessly fallen to the ground.
In reality, droplet models were just close range transmission, and airborne long range transmission of bio-aerosols, or micro droplets created from breathing, shouting, singing, coughing, or sneezing. The range was more a function of the transmissibility of the virus. Highly infective things can infect at low doses at long range. Less infective things occur with much higher doses, when people are quite close to one another. This folded in the prior models quite nicely. It was, however, not well accepted.
If a disease is to be transmitted by bio-aerosols, the disease vector needs to be able to enter the body through the surfaces with which it will interact upon being “breathed in”. This doesn’t work well for the STI viruses or bacteria, nor the malarial parasite, as they aren’t actively expelled in the respiratory system, so don’t generate bio-aerosols, and require access to highly specific host cells not easily accessed through the respiratory system at the necessary volumes to create an infection.
So, no, not really possible for non-respiratory viruses to become “airborne” in that sense.there would need to be a LOT of intermediate steps.
But diseases that we used to consider to be transmitted by the now defunct ballistic droplet model can become “airborne” (instead of “droplet”) if their ability to infect a subject becomes more successful at lower doses of pathogen such that it can occur at longer range, and over longer times.
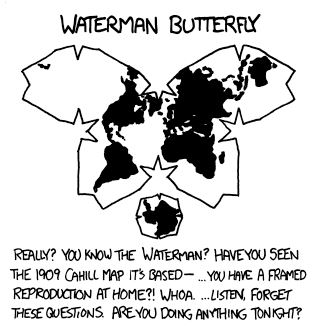
Like all maps, this one needs a date. For example, Canada and Denmark now share a land border (Hans island)
generate some minor descriptions for generic stuff in my TTRPG campaigns.
Need a quick 200 word description of the interior of an apothecary? Or a band of marauding orcs? It’s been a huge time saver for me.

3 Astronauts. 1 candidate. Only really got to know one astronaut (family friend) and one candidate (supervised her training in an unrelated field) super well. I’ve had long term interactions with two wannabes who were disasters.
Unfortunately, in contrast to astronauts, most of the politicians I’ve met are complete shits. Only met a few at the civic level who are excellent. And one at the federal level. Everyone else has been truly🤮.
It’s funny. Literally every astronaut I’ve met is exactly like this - quietly competent, affable, team player. As is the astronaut candidate I’ve met.
And yet…
Every person I’ve met who has been keen on becoming an astronaut or astronaut candidate has been an insufferable self-aggrandizing jerk face. Like, just awful people who suck all the air out of any room they’re in, expounding on how they (or the idea they’re selling) are the most amazing thing ever.

Most answers here are missing the benefits of a home Mac running 24/7 if you’re already part of the Apple ecosystem. For example, you can have it sync all your iCloud data (documents, photos, iTunes content) and back them up locally, then elsewhere outside of Apple’s ecosystem. You can also have it act as a local CDN for OS updates, whereby it will cache OS downloads locally so any subsequent updates will be super quick.
On the downside, I found native Docker on macOS kinda sucked, and just installed Ubuntu on my 2012 Mac Mini (now running Proxmox for funsies), but I have an old iMac to do the caching. You could probably virtualize and get both benefits, and I am considering moving to a new M4 mini for the power savings and sheer speed. That M4 Pro chip has absolutely incredible Geekbench numbers while sipping power.